Overtreatment in IVF: A Senior Fertility Specialist’s Perspective
By Prof. (Dr.) Abha Majumdar
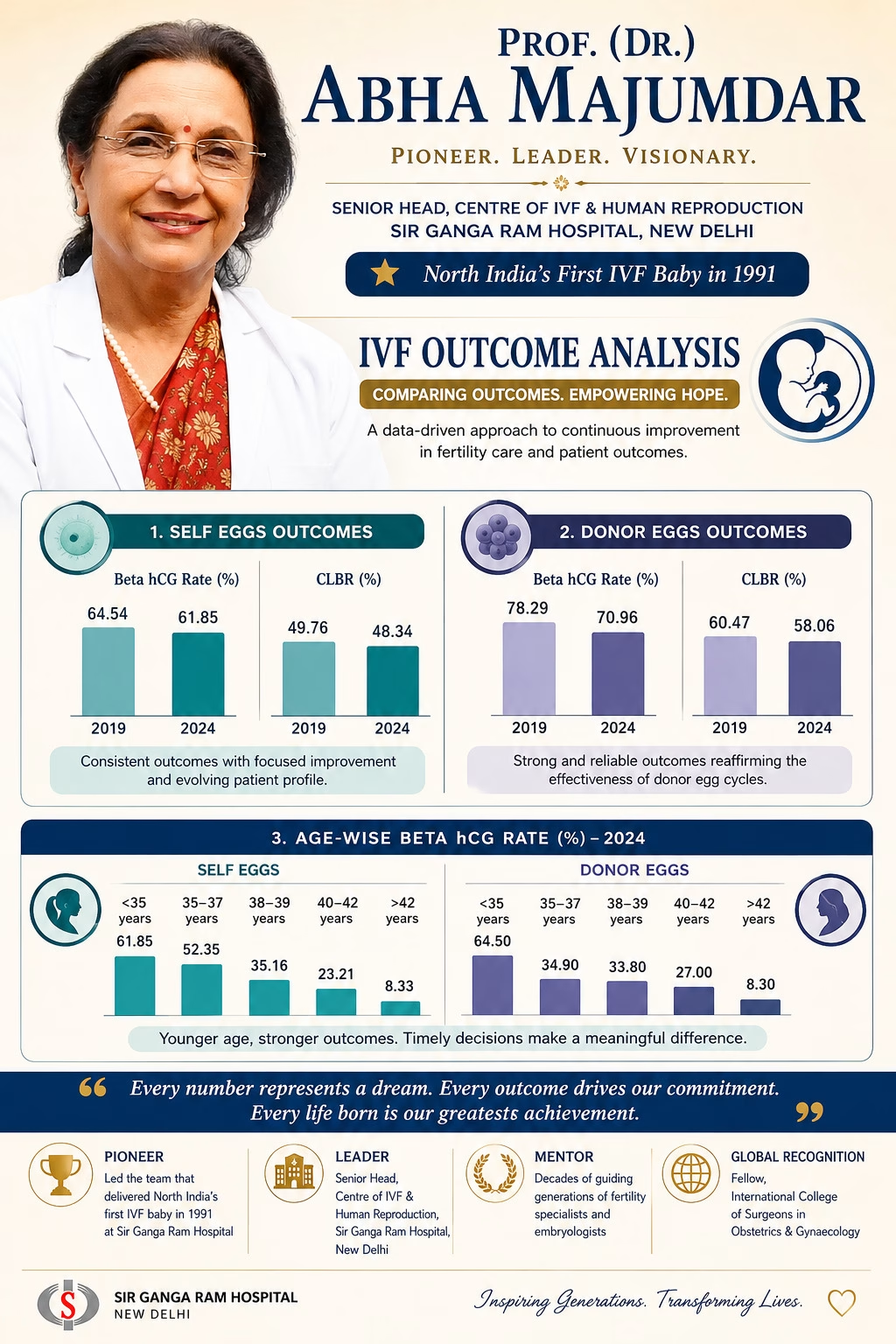
Having spent more than 40 years in reproductive medicine—and having had the privilege of helping deliver North India’s first IVF baby at Sir Ganga Ram Hospital in 1991—I have seen firsthand the incredible evolution of fertility treatments. While science and technology have advanced rapidly, one core principle must remain unchanged: Do what is necessary, not what is excessive.
This conviction is why we need an honest conversation about a growing concern in modern fertility care: overtreatment in IVF, specifically the routine use of unproven “treatment add-ons.”
When “More” is Mistaken for “Better”
In vitro fertilization (IVF) and intrauterine insemination (IUI) are established, core treatments that have been proven effective for most patients. However, overtreatment happens when we mistake more intervention for better care. It can take many forms:
Starting IVF too early, even when natural conception remains possible.
Ordering excessive investiga tions that create anxiety but do not change clinical outcomes.
Prescribing multiple medications without proven additional benefits.
Routinely recommending optional, non-essential “add-ons” under the assumption that they act as “implantation boosters.”
The very term ‘add-on’ suggests ‘extra benefit’. But medicine must be guided by evidence—not assumption. Leading regulators, such as the ‘Human Fertilization and Embryology Authority’ (HFEA for UK) have repeatedly highlighted that for most patients, routine cycles of proven fertility treatment are highly effective ‘without’ using any treatment add-ons.
Understanding the Evidence: The HFEA Traffic-Light Ratings
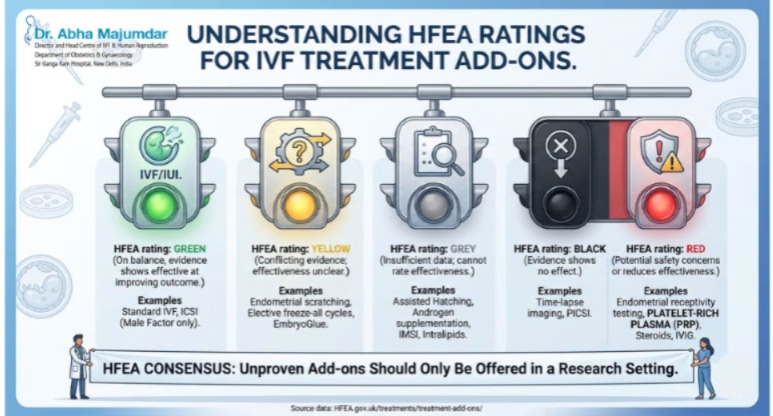
To protect patients and bring transparency to the field, the HFEA’s Scientific and Clinical Advances Advisory Committee (SCAAC) reviews published data and categorizes common add-ons using a strict traffic-light rating system.
When clinics routinely suggest these procedures, patients must understand where they stand on the scientific spectrum:
🟢 Green: High-quality evidence shows this add-on is effective at improving treatment outcomes. (Notably, no routine add-ons carry a green light for general use).
🟡 Yellow (Conflicting Evidence): It is not entirely clear if the add-on is effective because moderate-to-high-quality studies show conflicting results. Examples: endometrial scratching, elective freeze-all cycles, and Hyaluronate-enriched pre-transfer culture medium (e.g., Embryo Glue).
🔘 Grey (Insufficient Evidence): The effectiveness cannot be verified due to a lack of high-quality data. Examples: Assisted Hatching, Androgen supplementation, Intracytoplasmic morphologic sperm injection (IMSI), and Intralipids (immunological therapy).
⚫ Black (No Effect): Moderate-to-high-quality evidence explicitly shows this add-on has no effect on improving the treatment outcome. Examples: Time-lapse imaging a, and physiological intracytoplasmic sperm injection (PICSI).
🔴 Red (Safety Concerns / Decreased Effectiveness): High-quality evidence indicates potential safety risks or shows that the add-on may reduce the effectiveness of your treatment. Examples: Endometrial receptivity testing, steroids (Glucocorticoids), Intravenous immunoglobulin (IVIG), and Platelet-rich plasma (PRP) treatments (both intraovarian and intrauterine).
When is it Appropriate to Use a Treatment Add-on?
This evidence should make all of us pause, but it does not mean add-ons have no place in medicine. There are valid nuances to consider:
Justifiable Medical Redirection: An add-on may be offered for reasons other than simply increasing the live birth rate. For example, specific protocols might be justified if they significantly reduce the risk of a miscarriage such as with natural ovulatory cycle for frozen embryo transfer or mitigate the threat of Ovarian Hyperstimulation Syndrome (OHSS) in a specific high-risk patient by using antagonist protocol with agonist trigger and freeze all policy.
Strictly Monitored Subgroups: Certain procedures are authorized only for highly selected cohorts. For instance, ‘Artificial oocyte Activation by using Calcium Ionophore carries potential chromosomal risks and is not meant for routine use, but it may be justified for patients with specific cellular deficiencies (like PLC zeta deficiency) or those with severe, repeated fertilization failure.
Research, Not Retail: Treatments that lack strong evidence of safety or effectiveness ‘should only be offered within formal research setting or clinical trial’. Crucially, patients should never be charged extra to participate in research.
If you are paying out-of-pocket, it is frequently more effective to save those financial resources to fund a subsequent, clean routine IVF cycle rather than exhausting your savings on unproven add-ons for a single cycle.
The Rise of “Package-Driven” IVF
Compounding the issue of clinical overtreatment is the commercialization of fertility care. Today, vulnerable patients are frequently influenced by retail-style marketing: discounts, festival offers, “guaranteed packages,” and free gifts.
But IVF is a medical journey, not a retail transaction. A “cheaper package” headline often masks hidden lines. It may completely exclude:
Essential medications and stimulation hormones
Embryo freezing and long-term storage charges
Anesthesia and operating theatre fees
Advanced laboratory procedures or repeat ultrasound monitoring
These financial layers often appear later—at a point when patients are already emotionally and physically invested. Patients deserve absolute, unambiguous financial transparency from day one.
Empowering Couples: Questions to Ask Your Clinic
Before committing to a fertility clinic, look past the marketing and ask the hard, clinical questions:
What is your live birth rate, not just your chemical pregnancy rate?
What is your age-specific outcomes for someone like me?
Is this protocol being explicitly individualized for my unique condition, or is it a standard clinic protocol?
Why am I being recommended this specific add-on, and what specific evidence supports its use for my case?
What is the quality and accreditation of your embryology laboratory?
A good clinic explains; it does not pressurize. A good doctor informs; they do not frighten.
My Philosophy After Decades in IVF
Technology is valuable and innovation is welcome. But wisdom in reproductive medicine lies in knowing when not to intervene unnecessarily. My favorite quote as an ob./gyn and reproductive clinician which I have pragmatically followed all my life is ‘Masterly inactivity and timely intervention’.
Good IVF is not about doing the most; it is about doing what is right—for the right patient, at the right time, and for the right clinical reason. Patients are not purchasing a commercial product. They are placing their vulnerability, their trust, and their deepest dreams of parenthood into our hands. That trust must always be honored with rigorous science, uncompromised ethics, and genuine compassion.
Stem Cell Therapy for Severe Asherman’s Syndrome: Historical Success
A historic milestone in regenerative medicine: Prof. (Dr.) Abha Majumdar and her clinical team achieve India’s first successful live births utilizing umbilical cord-derived mesenchymal stem cells to reverse severe uterine scarring.
Stem Cell Therapy Enables India’s First Successful Births in Severe Asherman’s Syndrome
A historic breakthrough in reproductive regenerative medicine has opened transformative treatment possibilities for women facing complex uterine infertility barriers. Doctors at the prestigious Sir Ganga Ram Hospital in New Delhi have reported India’s first successful live births following stem cell therapy for severe Asherman’s Syndrome. This pioneering clinical milestone offers a powerful, scientifically validated alternative to couples previously left with limited reproductive choices.
This groundbreaking clinical trial and successful delivery management protocol were directed by Prof. (Dr.) Abha Majumdar, Director and Head of the Centre of IVF and Human Reproduction. Her expert medical team successfully utilized clinical-grade umbilical cord-derived mesenchymal stem cells to repair long-standing intrauterine scar tissue and safely restore endometrial function required for a full-term pregnancy.
Understanding Severe Asherman’s Syndrome
Asherman’s Syndrome is an intricate reproductive condition characterized by the formation of dense scar tissue (synechiae/adhesions) inside the uterine cavity. This structural damage often leads to partial or total obliteration of the uterine space. Clinically, these scarring patterns typically develop as secondary complications following invasive pelvic events:
Traumatic post-abortal or postpartum Dilation and Curettage (D&C) procedures.
Severe, deep-seated intrauterine infections (such as Endometrial Tuberculosis).
Complex intrauterine surgical interventions or myomectomies.
In extensive, severe variations of this syndrome, the structural basal layer of the endometrium is entirely destroyed. Consequently, the uterine lining loses its capacity to thicken or respond to natural hormonal stimulation. Until recently, women with flat, non-responsive linings faced complete reproductive barriers, forcing them to rely exclusively on surrogacy or adoption pathways.
The Scientific Innovation: How Stem Cell Therapy Works
To overcome this absolute tissue barrier, Dr. Abha Majumdar’s clinical protocol utilized high-potency mesenchymal stem cells harvested carefully from the Wharton’s jelly of the umbilical cord. These specialized cells are globally recognized for their exceptional anti-inflammatory, immunomodulatory, and cellular regenerative capacities.
The highly detailed micro-surgical clinical sequence involves three distinct phases:
Harvesting and Culture: Isolating clinical-grade mesenchymal stem cell populations derived safely from umbilical cord tissues.
Hysteroscopic Micro-Injection: Following surgical clearance of visible scar sheets, the cellular matrices are injected directly beneath the non-responsive basal layer under direct hysteroscopic visualization.
Endometrial Reconstruction: The injected cells stimulate localized angiogenesis (blood vessel formation) and actively rebuild a rich, vascularized endometrial tissue base.
By safely targeting the core basal layer, the regenerative treatment triggers natural cellular repair networks. This process successfully restores the uterine environment’s capability to safely accept, attach, and sustain a developing embryo.
Successful Births: Clinical Trial Case Outcomes
This dynamic breakthrough was achieved during a tightly controlled clinical trial monitoring ten patients diagnosed with advanced, severe forms of Asherman’s Syndrome. Out of the trial group, two patients have successfully delivered healthy babies after completing the intra-follicular tissue rejuvenation therapy:
Patient Profile
Baseline Uterine Status
Clinical Stem Cell Outcome
Delivery Metrics
Case 1: 39-Year-Old
Severe, dense intrauterine adhesions with complete cessation of menstrual cycles.
Successful reduction of scar layers; restoration of normal tissue elasticity.
Delivered a healthy baby boy at 35 weeks, weighing 2 kg.
Case 2: 40-Year-Old
Recurrent pregnancy loss paired with a permanently thin, damaged endometrial track.
Marked improvement in tissue vascularity and steady endometrial thickness growth.
Delivered a healthy baby girl at 31 weeks, weighing 1.8 kg.
Following the stem cell micro-infusion cycles, both trial participants achieved normal menstrual flows, sustained appropriate endometrial thickness metrics above critical thresholds, and experienced a massive reduction in adhesion recurrence vectors.
A Transformative Dawn for Reproductive Medicine
This therapeutic milestone demonstrates the immense clinical potential of regenerative medicine within modern fertility science. By actively reversing internal structural damage rather than simply bypassing it, stem cell protocols offer authentic hope to thousands of couples dealing with unexplained or structural uterine infertility.
As advanced global multi-center trials continue to confirm these safety and efficacy baselines, this specialized cell-infusion protocol is poised to become a core corrective option for severe intrauterine pathologies globally.
About Prof. (Dr.) Abha Majumdar
Prof. (Dr.) Abha Majumdar is widely regarded as an international pioneer in assisted reproductive technology (ART) and advanced pelvic microsurgery. As the Director and Head of the Centre of IVF and Human Reproduction at Sir Ganga Ram Hospital, she has spent decades resolving the most complex infertility cases. Notably, she was a key member of the historic medical team responsible for delivering the first successful IVF baby in North India in 1991.
Through her continuous contributions to academic clinical research and her dedication to evidence-based reproductive science, she remains committed to developing innovative treatments that turn the dream of parenthood into a reality for couples worldwide.
Understanding the IVF Process for Complex Medical Conditions
Understanding IVF: How In Vitro Fertilization Helps Women with Complex Medical Conditions
In contemporary reproductive medicine, building a family presents distinct physiological challenges for women navigating complex clinical diagnoses, advanced maternal age, or unexplained infertility factors. If you are facing these hurdles, In Vitro Fertilization (IVF) stands out as a highly specialized, reliable micro-assisted technology that has empowered millions of couples worldwide to realize their dreams of parenthood.
At the specialized private portal of Prof. (Dr.) Abha Majumdar, India’s leading fertility pioneer, we blend clinical precision with deeply individualized treatment protocols. Our medical team guides you safely through every step of this complex reproductive journey, ensuring your safety, physiological comfort, and highest statistical chance of clinical success.
What Is IVF? The Embryological Framework
In Vitro Fertilization (IVF) is a sophisticated clinical technique where maternal oocytes (eggs) and paternal spermatozoa (sperm) are fertilized outside the human body inside a highly monitored, state-of-the-art embryology laboratory. Following successful fertilization and blastocyst development, the resulting high-grade embryo is precisely transferred back into the patient’s uterine cavity, establishing the pathway for optimal implantation and a healthy, full-term pregnancy.
While standard public perception links IVF primarily to basic blocks, modern reproductive science utilizes custom iterations of this process to bypass severe systemic health conditions and metabolic disorders in female patients.
How IVF Bypasses Complex Female Medical Conditions
Systemic diseases and reproductive anomalies can deeply affect natural ovulation, fertilization, and embryonic travel. Below is a detailed scientific breakdown of how tailored IVF protocols address specific health conditions:
1. Polycystic Ovary Syndrome (PCOS)
PCOS is characterized by chronic anovulation and hyperandrogenism, creating erratic follicular development. During an IVF cycle, we implement customized, low-dose antagonist protocols paired with precise trigger mechanisms. This highly controlled ovulation induction allows us to retrieve healthy, mature eggs while completely eliminating the risk of Ovarian Hyperstimulation Syndrome (OHSS).
2. Endometriosis (Mild to Severe)
Endometriosis triggers extensive pelvic inflammation, anatomical distortions, and toxic peritoneal fluids that degrade egg quality and damage fallopian tubes. IVF completely bypasses these hostile pelvic environments by harvesting oocytes directly from the ovaries, managing fertilization in a protected laboratory, and preparing the uterine lining separately before a frozen transfer.
3. Unexplained Infertility Barriers
When standard diagnostic assessments yield completely normal results yet conception fails over years, subtle micro-factors like thick oocyte shells or sperm binding errors are often at play. IVF resolves these hidden barriers by providing direct cell interaction monitoring or utilizing Intracytoplasmic Sperm Injection (ICSI) to guarantee clear fertilization tracks.
4. Mechanical Fallopian Tube Blockage
Whether caused by pelvic inflammatory disease (PID), past tubal pregnancies, or surgical ligations, damaged fallopian tubes create an absolute physical barrier to natural conception. IVF completely bypasses the fallopian tubes, picking up mature eggs directly from the ovaries and placing the cultured embryo directly into the uterus.
5. Low Ovarian Reserve (Low AMH)
As the functional ovarian reserve naturally declines with age or due to premature ovarian insufficiency, maximizing every single cell becomes vital. Our center utilizes advanced mild stimulation cycles and dual-stimulation techniques to gather high-quality oocytes, and we offer perfectly matching donor egg frameworks when needed.
Systemic autoimmune conditions can create hostile endometrial environments due to hyperactive immune responses. IVF allows us to achieve pregnancy safely by stabilizing the patient’s condition during periods of low disease activity, freezing the embryos, and applying specialized immunomodulatory supportive therapies before the transfer cycle.
7. Epilepsy and Neurological Conditions
Managing pregnancy alongside anti-epileptic medications (AEDs) requires intense clinical caution due to potential medication interactions. A structured IVF plan ensures close monitoring, enabling safe pre-conception medication adjustments and carefully timed deliveries managed jointly with expert neurologists.
8. Age-Related Fertility Declines
Oocyte quality and chromosomal normality decline rapidly after the age of 35. To safeguard outcomes for advanced maternal age couples, our IVF setups combine precise cell cultivation with Preimplantation Genetic Testing (PGT-A), identifying chromosomally normal embryos to maximize live birth percentages.
Chemotherapy and pelvic radiation treatments can drastically deplete or destroy a patient’s ovarian reserve. Working closely with oncologists, we provide rapid-cycle random-start egg freezing or embryo vitrification before cancer treatments begin, preserving your future options for building a family after recovery.
Clinical Excellence & Patient Care Standards
Prof. (Dr.) Abha Majumdar brings over three decades of advanced reproductive expertise to every treatment plan. Recognizing that no two patients share identical metabolic or structural realities, our center avoids assembly-line treatment models in favor of highly personalized, data-driven medical protocols.
Operating out of the globally acclaimed Sir Ganga Ram Hospital, our laboratory systems maintain the highest clinical standards. From comprehensive pre-treatment counseling to protective post-procedure care, we ensure you receive transparent, compassionate, and cutting-edge medical support.
Why Select Dr. Abha Majumdar’s Team for Your IVF Care?
Tailored Protocol Designs: Every hormonal dose, lifestyle advice, and lab selection is customized to fit your specific biological profile.
Academic Leadership: Dr. Abha Majumdar was a key leader on the historic medical team that delivered the first successful IVF baby in North India in 1991.
Advanced Laboratory Infrastructure: Access to state-of-the-art technologies, including Next-Generation Sequencing (NGS), laser-assisted hatching, and high-definition vitrification tracking systems.
Compassionate, Ethical Care: We maintain complete medical transparency, prioritizing patient safety and evidence-based medicine above commercial targets.
Conclusion: Take the First Step Toward Your Family
Navigating infertility alongside complex medical challenges requires more than standard care; it demands world-class clinical expertise and genuine dedication. Dr. Abha Majumdar and her specialist team are ready to guide you through a safe, predictable, and exceptionally managed path toward parenthood.
Schedule Your Clinical Evaluation Today. Contact our administrative team to book your consultation and explore your personalized fertility options. Let us help turn your dreams of parenthood into a beautiful reality. 💕✨
📺 Media Broadcast: Watch the complete clinical panel discussion aired exclusively on Zee News Network.
IVF: Science, Hope & The Future of Fertility – A Media Interaction with Dr. Abha Majumdar & Dr. Neeti
In a rapidly progressing global healthcare landscape, reproductive endocrinology continues to scale new heights, providing highly scalable clinical alternatives where traditional pathways face limitations. A key pillar among these modern innovations is In Vitro Fertilization (IVF)—a highly structured micro-assisted reproductive procedure that has successfully transformed millions of families worldwide.
In an exclusive television interaction broadcast by Zee News, India’s foremost fertility pioneer Prof. (Dr.) Abha Majumdar, working alongside clinical reproductive expert Dr. Neeti, addressed the public to demystify advanced embryological protocols, separate facts from societal misconceptions, and outline the emotional architecture of modern fertility cycles.
Demystifying the Advanced IVF Lifecycle
Modern IVF has evolved from a misunderstood, highly restricted procedure into an accessible, highly calculated clinical sequence for couples facing complex conception blocks. As explained during the broadcast, a standard controlled cycle follows a rigid four-stage medical protocol:
Controlled Ovarian Stimulation: Administering precisely calculated hormonal regimens over 10 to 12 days to safely induce the growth of multiple high-quality maternal oocytes (eggs).
Ultrasound-Guided Egg Retrieval: A minor, completely painless outpatient micro-procedure performed under light sedation to safely extract mature oocytes from follicular fluids.
Laboratory Fertilization (Embryogenesis): Introducing the harvested oocytes to optimized paternal sperm cells within highly monitored incubator environments using advanced conventional methods or Intracytoplasmic Sperm Injection (ICSI).
Strategic Embryo Transfer: Transferring top-grade blastocysts directly into a perfectly synchronized, highly receptive uterine wall to establish optimal implantation pathways.
A major point clarified during the interview is that post-transfer care does not require complete or absolute bed rest. Patients are fully encouraged to safely resume their normal daily tasks while maintaining a few basic, healthy lifestyle modifications.
Primary Success Parameters in Assisted Reproduction
Addressing core success variations, Dr. Neeti highlighted that maternal biological age and functional ovarian reserve (indicated via AMH testing) remain the primary baseline indicators for initial cycle outcomes. Female patients under the age of 35 typically register significantly higher success rates due to a greater reserve of chromosomally normal eggs.
However, the panel strongly emphasized that fertility is a shared journey. Paternal semen factors—including sperm count, advanced motility dynamics, and DNA fragmentation indices—critically impact blastocyst development rates. Furthermore, high systemic stress levels can negatively influence hormonal balance, making comprehensive psychological support essential for achieving optimal outcomes.
The Evolution of Social Egg Freezing
A key focus of the television discussion centered on the rising adoption of Social Egg Freezing (Oocyte Vitrification). Modern career timelines and personal milestones often prompt women to safely delay family planning. This advanced preservation technique enables women to secure their prime reproductive cells during their peak biological years for use in future transfer cycles.
Professor’s Professional Quote: Social egg freezing represents a major advancement in reproductive autonomy. It provides women with a reliable scientific tool to protect their fertility choices, effectively neutralizing the pressures of the biological clock until they feel completely ready for motherhood.
Navigating the Complete Care Landscape
The panel highlighted that undergoing a fertility cycle involves a complete mental, physical, and financial commitment. Navigating unexpected cycle shifts or past failures requires immense resilience, clear clinical guidance, and professional counseling to protect patient well-being.
Because top-tier fertility care utilizes highly complex laboratory technologies, couples should always select established institutional centers. Partnering with trusted experts ensures complete transparency regarding diagnostic pathways, safety guidelines, and treatment costs before starting a cycle.
Normalizing Fertility Management: Removing the Taboo
The core message of the broadcast focused on removing outdated societal stigmas around fertility care. As public awareness grows, advanced reproductive treatments are no longer viewed as a confidential last resort, but as a standard, scientifically validated solution to a recognized medical condition.
Both Dr. Abha Majumdar and Dr. Neeti continue to champion transparent community conversations, encouraging families to embrace modern science-backed choices to experience the beautiful journey of parenthood.
IVF and Emotional Health: The Invisible Journey
📽️ Video Message: Watch Prof. (Dr.) Abha Majumdar’s full message on emotional resilience.
IVF and Emotional Health: A Message Every Woman Needs to Hear
By Prof. (Dr.) Abha Majumdar | Infertility Specialist
💬 “IVF is not just a medical procedure—it’s an emotional journey.”
While In-Vitro Fertilization (IVF) offers a beacon of hope for couples struggling with infertility, it also brings with it a heavy emotional toll—something that often goes unnoticed or unspoken.
In a powerful message, Dr. Abha Majumdar, one of India’s leading infertility specialists, highlights the deep emotional stress couples endure during IVF—especially when results don’t go as planned.
💔 The Emotional Reality of IVF
For most couples, IVF is not the first step—it’s often the last resort after months or years of trying to conceive naturally. By the time they reach this stage, they’re already emotionally vulnerable.
But IVF is not just about injections, scans, and transfers.
It’s about waiting—endlessly.
It’s about hope rising and falling with each cycle.
It’s about the physical pain, hormonal shifts, and financial burden.
And when it doesn’t work, it feels like a personal failure, even though it’s not.
🩺 What Happens When IVF Fails or Pregnancy Has Complications?
When an IVF attempt results in a negative pregnancy test, or a pregnancy ends in complications like bleeding or miscarriage, the emotional toll multiplies.
Dr. Majumdar says:
“In natural conception, couples can process the stress a bit more spontaneously. But in IVF, every attempt involves months of planning, physical exertion, emotional commitment, and substantial financial investment. When the result is negative—or worse, a pregnancy ends unexpectedly—the grief is amplified.”
👩❤️👨 It’s Not Just the Woman—The Couple Suffers
Often, emotional support focuses only on the woman. But IVF impacts both partners.
Men may feel helpless, not knowing how to support their wives.
Women may feel isolated, assuming their emotions are “too much.”
Both may experience relationship strain, especially with repeated cycles or failed outcomes.
🧘♀️ The Importance of Emotional Support
Medical treatment is just one part of the fertility journey. What many couples truly need is:
Psychological counseling to manage stress and anxiety.
Support groups to connect with peers facing similar journeys.
Compassionate care from their clinical fertility team.
Open conversations with trusted family and friends.
Dr. Majumdar encourages families to create a safe space for women going through IVF—to validate their emotions and acknowledge their strength.
💡 A Final Word of Encouragement
To every woman or couple going through this: You are not alone. Your emotions are valid. Your resilience is real.
Whether you’re starting your first cycle, recovering from a failed one, or holding your breath after a positive test—you deserve support, understanding, and care.
💙 There is strength in being vulnerable. There is power in being heard.
IVF Baby ≠ C-Section: Vaginal Delivery Realities
IVF Baby ≠ C-Section Delivery: Busting the Myth with Science
By Prof. (Dr.) Abha Majumdar | Director & Head, Centre of IVF, Sir Ganga Ram Hospital
There is a widely circulated, non-medical myth in society suggesting that if a baby is conceived through In-Vitro Fertilization (IVF), the mother must automatically deliver via a C-section (Cesarean section). This deep-rooted misconception often generates unnecessary anxiety, fear, and psychological stress for expectant families during their fertility journeys.
Core Medical Fact: IVF conception does not mandate a C-section delivery. The method of conception—whether spontaneous natural fertilization or advanced assisted reproduction—has absolutely no medical bearing on the clinical selection of the delivery pathway.
IVF Does Not Equal Cesarean: The Clinical Reality
Your physiological capability to achieve a normal vaginal delivery depends entirely on standard obstetric and maternal-fetal factors, rather than laboratory fertilization. The core clinical metrics evaluated during late-term gestation include:
Fetal Presentation: The structural alignment and positioning of the baby within the uterus.
Uterine Efficiency: The baseline health, readiness, and progressive dilation capability of the cervix.
Pelvic Architecture: The physical adequacy and diameters of the maternal pelvis relative to the fetal head.
Gestation Progression: The overall metabolic and physical health indicators of both mother and child during third-trimester monitoring.
If all physiological indicators align favorably, an IVF mother is an excellent candidate for a safe, spontaneous vaginal birth.
5 Structural Criteria for a Normal Vaginal Delivery
Obstetric teams utilize data-driven indices to evaluate maternal candidacy for normal delivery, irrespective of past fertility interventions:
1. Active Prenatal Conditioning
Mothers who maintain continuous, doctor-approved physical activity during pregnancy establish optimized muscle tone, superior stamina, and balanced weight metrics—all of which actively aid the natural labor sequence.
2. Cephalic Fetal Presentation
A standard head-down (cephalic) position as the baby approaches the pelvic inlet is the ideal anatomical orientation required for normal labor progression.
3. Optimized Fetal Macrosomia Metrics
When the baby’s estimated structural weight falls within standard normal parameters, vaginal delivery is heavily favored. Excessively large baby sizes (fetal macrosomia) may require a planned surgical intervention purely for maternal-fetal safety.
4. Proportionate Pelvic Pelvimentry
An adequate, uncompromised maternal pelvic passage ensures sufficient internal clearance for the baby to transition safely through the birth canal without mechanical obstruction.
5. Absence of Critical Gestational Complications
In the documented absence of secondary high-risk medical alerts—such as placenta previa (low-lying placenta), severe pre-eclampsia (pregnancy-induced hypertension), or acute fetal distress—vaginal labor remains the primary clinical choice.
What Truly Dictates the Mode of Delivery?
When separating clinical evidence from outdated cultural myths, the determination to perform a C-section is strictly restricted to active systemic variables, including:
Maternal biological age and general metabolic health profiles.
History of prior complex uterine surgeries or previous classical cesarean sections.
Cervical non-readiness or failure of labor progression over time.
Assisted Conception Does Not Imply Maternal Fragility
An unfortunate stereotype often labels IVF mothers as too “fragile” or clinically sensitive to tolerate natural labor. This is biologically incorrect. IVF is simply a scientific tool designed to bridge the initial conception gap. Once implantation is successfully achieved, the subsequent gestational development is identical to natural pregnancy.
An IVF pregnancy is just as resilient, the maternal body is just as capable, and the inherent physiological mechanics required for normal delivery are just as powerful.
The Clinical Takeaway
It is time to systematically dismantle outdated social taboos surrounding reproductive science. IVF is an innovative blessing, not a medical restriction. If your baseline health parameters are optimal, your stamina is strong, and your fetal presentation is cephalic, opting for a normal delivery is a highly realistic goal.
Understanding Infertility: Clinical Causes, Myths, and Treatment Reality
By Prof. (Dr.) Abha Majumdar | Director & Head, Centre of IVF, Sir Ganga Ram Hospital
Infertility remains one of the most misunderstood medical conditions globally—often heavily clouded by social stigma, cultural pressure, and metabolic misinformation. Globally, estimates suggest that approximately 1 in every 6 couples of reproductive age experience some form of conception delay during their lifetime. Navigating this challenge requires a solid foundation of scientific facts rather than societal assumptions.
What Is Infertility? The Clinical Definition
In reproductive medicine, infertility is classified as a specific medical condition affecting the reproductive system of either the male or female partner, or both. Clinically, it is diagnosed as the inability to achieve a successful pregnancy after 12 months or more of regular, unprotected sexual intercourse. The underlying causes vary dynamically: they may stem from maternal factors, paternal factors, a combination of both, or may be categorized as unexplained infertility after initial diagnostic screening.
Various health parameters, genetic traits, and lifestyle choices can directly impact reproductive capacity. Fortunately, proper education, timely diagnostic testing, and specialized interventions—such as Intrauterine Insemination (IUI) and In-Vitro Fertilization (IVF)—provide highly effective pathways for couples looking to build their families.
Infertility and Social Stigma: Overcoming Gender Inequality
Beyond the biological hurdles, infertility introduces a heavy emotional and social burden, particularly within deeply traditional socio-cultural settings like India. Despite clear medical data showing that reproductive challenges affect both sexes, a highly biased social perception often treats infertility as an exclusively female problem.
This systemic misunderstanding leads to immense emotional distress, anxiety, isolation, and low self-esteem for women. Addressing infertility openly as a shared, treatable medical condition is essential for promoting gender empathy and dismantling harmful societal taboos.
Busting Common Infertility Myths with Medical Facts
Dismantling common misconceptions allows couples to skip ineffective alternative routes and seek appropriate, evidence-based medical care early on:
❌ Myth: Infertility is almost always a woman’s biological issue.
Medical Fact: Infertility affects men and women equally. Clinical statistics show that paternal factor infertility accounts for approximately 50% of all documented cases, either as the sole diagnostic cause or alongside maternal factors. Comprehensive evaluation must involve both partners simultaneously.
❌ Myth: If you “just relax” and reduce stress, conception will happen naturally.
Medical Fact: While extreme stress can negatively alter hormonal balances, clinical infertility is rooted in concrete physical barriers (such as blocked fallopian tubes, low sperm counts, or ovulatory disorders). These conditions require targeted medical intervention, not just relaxation techniques.
❌ Myth: IVF is the immediate, only treatment option, and it works 100% of the time.
Medical Fact: IVF is an advanced reproductive milestone, but it is rarely the first or only treatment option. Many couples conceive using simpler first-line therapies, including ovulation induction medications, corrective surgeries, or structured IUI procedures. IVF success rates vary based on maternal biological age, ovarian reserves, and overall health profiles.
Modern Clinical Treatment Options for Couples
Advancements in reproductive endocrinology offer a wide range of treatment options customized to each couple’s unique diagnostic profile:
Targeted Lifestyle Modifications: Optimizing BMI, regulating metabolic function, and eliminating toxins to enhance baseline gamete quality.
Hormonal and Ovulation Medications: Prescribing precise therapies to stimulate healthy egg development and release.
Corrective Reproductive Surgery: Utilizing advanced minimally invasive laparoscopy or hysteroscopy to clear physical blockages or repair reproductive anatomy.
Assisted Reproductive Technology (ART): Utilizing precise laboratory procedures like IUI (placing washed sperm directly inside the uterus) or advanced IVF/ICSI sequences for complex cases.
Empowerment Through Open Conversations
Education is our most powerful tool for breaking down historical stigmas. By understanding the objective medical facts of human reproduction, couples can avoid unnecessary self-blame, seek professional guidance without hesitation, and make informed choices for their future families.
Amenorrhea (Missed Periods): Causes & Treatment
Clinical Clinical Guidelines • Patient Awareness
Amenorrhea: Understanding Causes, Types, Evaluation, and Management
A comprehensive clinical overview of absent menstrual cycles, neuroendocrine disruptions, and reproductive pathways
What You Need to Know About Amenorrhea
Amenorrhea is the medical term used when a woman or adolescent girl does not experience menstruation. While missing a menstrual cycle can occur due to entirely natural physiological milestones—such as pregnancy, lactation, or menopause—it frequently acts as an underlying symptom of deeper systemic issues. These can range from complex hormonal imbalances and high neuro-stress markers to rapid body mass fluctuations and intensive physical training overexertion.
Identifying the root cause of an absent cycle is crucial, as the regular rhythm of the menstrual cycle serves as a key indicator of overall metabolic, endocrine, and bone density health. Evaluation typically involves targeted hormone profiling panels, pelvic diagnostic imaging scans, and, where clinically relevant, detailed genetic mapping analyses.
⚠️ Clinical Indicator: If you have previously experienced regular cycles but your period has suddenly ceased for 3 consecutive months (or 6 months if your cycle was highly irregular), medical guidelines recommend scheduling a specialized evaluation rather than waiting for natural recovery.
Etiological Classification & Types
In clinical workflows, amenorrhea is categorized into two primary manifestations based on a patient’s medical and developmental history:
Primary Amenorrhea: The complete failure of menstruation to initiate by age 15 in the presence of expected secondary sexual characteristics (such as typical breast and pubic hair development). (Clinical Alert: Investigations must begin promptly by age 13 if secondary sexual characteristics are entirely absent | Agar 13 saal ki umra tak sharirik badlav shuru na hon, toh turant janch karani chahiye)
Secondary Amenorrhea: The cessation of menstruation for 3 consecutive cycles in individuals with previously regular periods, or for a continuous duration of 6 months in individuals with a history of irregular cycles.
Functional Hypothalamic Amenorrhea (FHA): Suppression of the body’s metabolic signaling pathway due to intense emotional stress, low caloric availability, or rigorous athletic overtraining.
Hyperprolactinemia: Elevated serum prolactin levels, often caused by microadenomas or specific neurological prescriptions.
Sheehan Syndrome: Ischemic necrosis of the pituitary gland caused by severe obstetric hemorrhage during delivery.
Intracranial Lesions: Structural anomalies like craniopharyngiomas or germinomas.
Polycystic Ovary Syndrome (PCOS): A highly prevalent endocrine disorder causing chronic anovulation and hyperandrogenism.
Primary Ovarian Insufficiency (POI): Premature depletion of ovarian follicles before reaching age 40 due to autoimmune, idiopathic, or toxic exposures.
Turner Syndrome (45,X): A major chromosomal abnormality causing dysgenetic streak ovaries.
Androgen Insensitivity Syndrome (AIS): A genetic variant where individuals with XY chromosomes exhibit variations in male androgen receptor sensitivity.
3. Uterine & Outflow Tract Abnormalities
Müllerian Agenesis (MRKH Syndrome): Congenital absence of the uterus, cervix, and upper vaginal structures.
Anatomical Obstructions: Structural congenital blocks like a transverse vaginal septum or an imperforate hymen.
Asherman Syndrome: Severe intrauterine adhesions and scarring within the endometrial cavity, often caused by past instrumentation or infections.
Clinical Evaluation Framework
A systematic diagnostic approach ensures accurate localization of the root cause along the hypothalamic-pituitary-ovarian-uterine axis:
Evaluation Category
Diagnostic Interventions & Medical Objectives
History & Physical Examination
Tracking baseline growth charts, family menarche patterns, evaluating Tanner staging (breasts/pubic hair), and screening for signs like sudden headaches or unexpected galactorrhea.
Targeted Laboratory Diagnostics
Serum Beta-hCG (to rule out pregnancy first), FSH, LH, Estradiol, Prolactin, TSH, Free T4, and Serum Testosterone/DHEA-S profiles. Karyotyping is reserved for clear primary presentation cases.
Advanced Diagnostic Imaging
High-resolution Pelvic Ultrasound to assess internal reproductive structures, Brain MRI for suspected central pituitary issues, and diagnostic Hysteroscopy for suspected intrauterine scarring.
Evidence-Based Management Protocols
Treatment strategy is dictated entirely by the localized clinical diagnosis:
Hyperprolactinemia: Targeted medical therapy utilizing specific dopamine agonists such as Cabergoline or Bromocriptine.
PCOS & Metabolic Concerns: Strategic weight reduction programs, cycle management via low-dose oral contraceptives, and insulin-sensitizing therapies like Metformin.
Primary Ovarian Insufficiency (POI): Timely initiation of Hormone Replacement Therapy (HRT) to safeguard bone mineral density and cardiovascular health.
Anatomic Outflow Track Anomalies: Specialized micro-surgical corrections (e.g., hymenotomy, septum resection, or hysteroscopic adhesiolysis for Asherman Syndrome).
Highest Success Rates in IVF – Myth or Fact?
Patient Awareness Published: February 15, 2025 • Editorial by Dr. Abha Majumdar
“Highest Success Rates in IVF” – Myth or Fact?
📢 Note: यह लेख डॉ. आभा मजूमदार द्वारा जनहित और मरीज जागरूकता के लिए पहले पब्लिश किए गए मूल चिकित्सा कॉलम (Original Medical Column) का संशोधित और पुनः प्रकाशित (Republished) संस्करण है।
Fact (With a Catch!) – IVF success rates can be exceptionally high, but they are highly variable and never uniform. Real success values fluctuate dramatically based on maternal age, severe physiological factors, the embryo laboratory’s specific technical setup, and individual health markers. While top-tier facilities legitimately register above-average outcomes, patients must remain highly cautious of sweeping, unverified promotional percentage statistics.
Common Myths vs. Facts About IVF Success Rates
❌ Myth: “IVF guarantees a positive pregnancy target.”
✅ Fact: IVF significantly optimizes fertilization odds but cannot offer absolute guarantees. Complete success relies heavily on background biological sync points, including gamete health, genetic structural integrity, and deep uterine endometrial thickness.
❌ Myth: “A facility broadcasting the highest success rate is automatically your best option.”
✅ Fact: Be careful. Certain facilities selectively filter data streams by processing only uncomplicated, high-prognosis patients to artificially keep statistics elevated. It is critical to investigate exactly how a center tracks its cumulative live-birth percentages. (Meaning: Some commercial clinics turn away tough cases to keep their success score looking high | Kuch clinics mushkil cases nahi lete taaki unka success rate papers par zyada dikhe)
❌ Myth: “IVF calculation benchmarks apply uniformly to all patients.”
✅ Fact: Biological realities dictate otherwise. Age remains the single most critical factor; women under 35 typically witness a baseline ~50% pregnancy rate per primary cycle, whereas success metrics gradually adjust as biological timelines advance.
❌ Myth: “The very first operational IVF loop must deliver success.”
✅ Fact: It is quite common for couples to require multiple sequential stimulations or staggered embryo transfers to secure a healthy clinical pregnancy. Patient persistence combined with clinical fine-tuning routinely opens up better developmental windows.
❌ Myth: “Fresh embryonic transfers yield superior results over frozen samples.”
✅ Fact: Advanced cryopreservation techniques mean Frozen Embryo Transfers (FET) match, and often exceed, fresh cycle success rates. This is because transferring frozen embryos allows the uterine lining to recover from intense stimulation hormones.
❌ Myth: “IVF procedures always result in twin or triplet births.”
✅ Fact: Modern embryology focuses heavily on Elective Single Embryo Transfer (eSET). This approach prioritizes healthy, full-term singleton deliveries while minimizing the medical risks associated with high-order multiple pregnancies. (Meaning: Intentionally transferring one premium embryo safely protects mother and child | Ek hi swasth embryo transfer karne se judwa bacho ke jokhimm ko kam kiya jata hai)
❌ Myth: “Daily baseline metabolic choices and dietary habits have no sway over outcomes.”
✅ Fact: Balanced nutritional plans, active weight management, and lowered cortisol stress markers distinctly protect cellular health and early implantation environments. Avoiding nicotine, chemical additives, and high-preservative processed items remains a medical necessity.
🔍 What to Critically Verify in an IVF Treatment Centre:
Clear and honest success rate reports categorized transparently by maternal age groups.
Active, in-house technical support for advanced procedures like ICSI, PGT diagnostics, and vitrification.
Comprehensive and patient-specific baseline diagnostic workups prior to starting stimulation cycles.
📞 Take a Transparent, Scientifically Sound Step Towards Parenthood
Holistic Support Published: February 20, 2025 • Written by Dr. Abha Majumdar
The Role of Yoga and Physical Exercises in IVF: Benefits and Limitations
Introduction
In-vitro fertilization (IVF) is an intricate, highly specialized, and often emotionally taxing journey for couples managing infertility concerns. Seeking to optimize their success corridors, many individuals incorporate holistic wellness modalities like yoga and regular low-impact exercise routines into their preparation timelines. While maintaining physical activity yields distinct systemic advantages, understanding its precise clinical limits inside the IVF framework is vital. This guide outlines where focused exercises actively support the reproductive tract and where medical pathology must take full precedence.
How Yoga and Physical Exercises Help in IVF
While supplementary routines can never replace primary embryology tracks, integrating tailored physical movements helps cultivate optimal conditions for IVF therapy in several key areas:
💪 Clinical Advantages & Physiological Assets
Reduces Stress and Chronic Anxiety: Navigating fertility treatments raises stress responses, producing elevated cortisol and adrenaline levels that can negatively disrupt delicate neuroendocrine signaling pathways. Restorative yoga balances this nervous response via controlled diaphragmatic deep breathing, target mindfulness, and meditation.
Improves Blood Circulation to Reproductive Organs: Select low-impact stretches actively minimize pelvic vascular resistance, channeling oxygenated blood flows directly toward the uterine walls and ovarian regions. Poses such as the Butterfly Pose and Legs-Up-the-Wall safely assist localized pelvic perfusion.
Supports Hormonal Homoeostasis: Regular physical activity assists in modulating endocrine functions, aiding the body’s natural management of estrogen, progesterone, and metabolic insulin levels. This metabolic stability is especially beneficial for patients managing Polycystic Ovary Syndrome (PCOS) or chronic cycle variations.
Enhances Endometrial Implantation Potential: Minimizing overall systemic inflammatory baselines creates a more receptive, relaxed uterine vascular matrix, which supports early embryo attachment.
Stabilizes Emotional Well-Being: The multiple phases of hormonal stimulation injections and the subsequent waiting intervals can be emotionally testing. Dedicated meditative exercises cultivate mental resilience, keeping couples grounded and positive throughout treatment.
Where Yoga and Physical Exercises are Not Effective in IVF
Despite clear therapeutic values for stress reduction, exercise routines cannot alter or resolve absolute structural, genetic, or physiological fertility blockages. Medical intervention remains essential for conditions such as:
⚠️ Pathological Realities & Limits
Structural Reproductive Track Blockages: Exercises cannot open fallopian tubes blocked by dense scar tissue, hydrosalpinx, or deep pelvic adhesions. Similarly, structural uterine anomalies like submucosal fibroids or endometrial polyps require formal hysteroscopic or laparoscopic surgical correction.
Chromosomal and Genetic Abnormalities: Structural chromosomal variations or genetic errors within embryos cannot be altered by lifestyle changes. Resolving recurrent implantation failures due to genetic factors requires advanced Embryology laboratory diagnostics like Preimplantation Genetic Testing (PGT).
Severe Oocyte or Sperm Quality Depletion: If a patient exhibits diminished ovarian reserve with low Anti-Müllerian Hormone (AMH) values, physical therapies cannot restore or create new primordial follicles. Likewise, absolute male factor concerns like severe sperm DNA fragmentation or azoospermia necessitate advanced micro-manipulation treatments like ICSI.
Autoimmune and Immunological Implantation Factors: Conditions involving systemic immune activation, such as systemic lupus erythematosus (SLE) or antiphospholipid syndrome (APS), cause immune-mediated rejection risks at the decidual lining. While exercise limits general metabolic inflammation, specific immune-modulating drug protocols are required to safeguard the embryo.
Age-Related Ovarian Atrophy: Natural chronological aging alters egg quality and cellular energy capacities within the ovaries. This biological reality cannot be reversed by physical lifestyle adjustments. Advanced age protocols or donor oocyte tracking often become the recommended paths for patients over 40.
Conclusion
Yoga and structured physical exercises serve as excellent complementary therapies that safely reinforce IVF frameworks by lowering stress markers, balancing metabolic pathways, and boosting healthy pelvic blood flow. However, they cannot override objective clinical pathologies like anatomical blocks, cellular genetic factors, or advanced ovarian aging. Combining mindful physical care with evidence-based reproductive medicine offers the most reliable, balanced path to a successful pregnancy.
Sir Ganga Ram Hospital
Rajendra Nagar
New Delhi, India-110060.
Email: ivfsgrh@gmail.com
Genesis Clinic
F-431, New Rajendra Nagar,
Landmark: Shankar Road Main Market, New Delhi -110060 For Appointment Only
011-45011438 (9 AM – 4 PM) +91-9810821594, 8375990881 Emergency Inquiry Only +91 8375990881
+91-9958076534 (4 PM – 9 PM)
+91-8447320605 Email:abhamajumdar@hotmail.com