The Scientific Truth About IVF Add-Ons: Evidence-Based Consensus directed by Prof. (Dr.) Abha Majumdar.
As couples research assisted reproduction online, they frequently encounter an array of supplementary laboratory procedures marketed as “IVF Add-Ons.” To clear this confusion, Prof. (Dr.) Abha Majumdar breaks down the genuine scientific data to separate commercial marketing from true clinical value.
What Exactly Constitutes an IVF Add-On?
An “add-on” refers to any optional medical or laboratory technology introduced alongside a standard IVF cycle to theoretically enhance success. While these procedures claim to boost implantation rates, many options lack large-scale, independent scientific validation. Consequently, applying them routinely to every patient adds unnecessary financial costs without delivering real clinical benefits.
However, when utilized selectively for specific diagnostic conditions, certain add-ons provide valuable support. An evidence-based approach avoids a one-size-fits-all model. Therefore, evaluating options through an objective, scientific framework is vital to protect ones treatment safety and transparency.
Evidence-Based Matrix of Common IVF Add-Ons
To help you understand their real clinical utility, this matrix evaluates common add-ons using international scientific standards:
Laboratory Add-On
How It Claims to Work medically
The Real Scientific Consensus
EmbryoGlue
An enrichment medium high in hyaluronan designed to help the embryo adhere to the uterine wall.
Shows moderate evidence of benefit in cases of previous unexplained implantation failures.
Laser Hatching
A precision laser creates a tiny opening in the outer shell (zona pellucida) of the embryo.
Highly useful for older patients with thickened embryo shells or when using frozen-thawed embryos.
Artificial Oocyte Activation (AOA)
Utilizes specialized calcium ionophore solutions to trigger egg activation during ICSI procedures.
Strictly indicated only for severe paternal factor cases with previous fertilization failures.
Before consenting to any optional addition, ask your medical team for independent clinical trial data supporting that specific technique. Ensure the option safely matches your exact diagnostic needs rather than generic trends. Making decisions based on clear, scientific evidence protects your peace of mind throughout your journey.
Ultimately, a successful IVF treatment relies on excellent baseline embryology, optimal uterine preparation, and personalized care. By keeping our protocols rooted in honest, peer-reviewed science, we protect couples from commercial exploitation while delivering the highest standard of modern reproductive care.
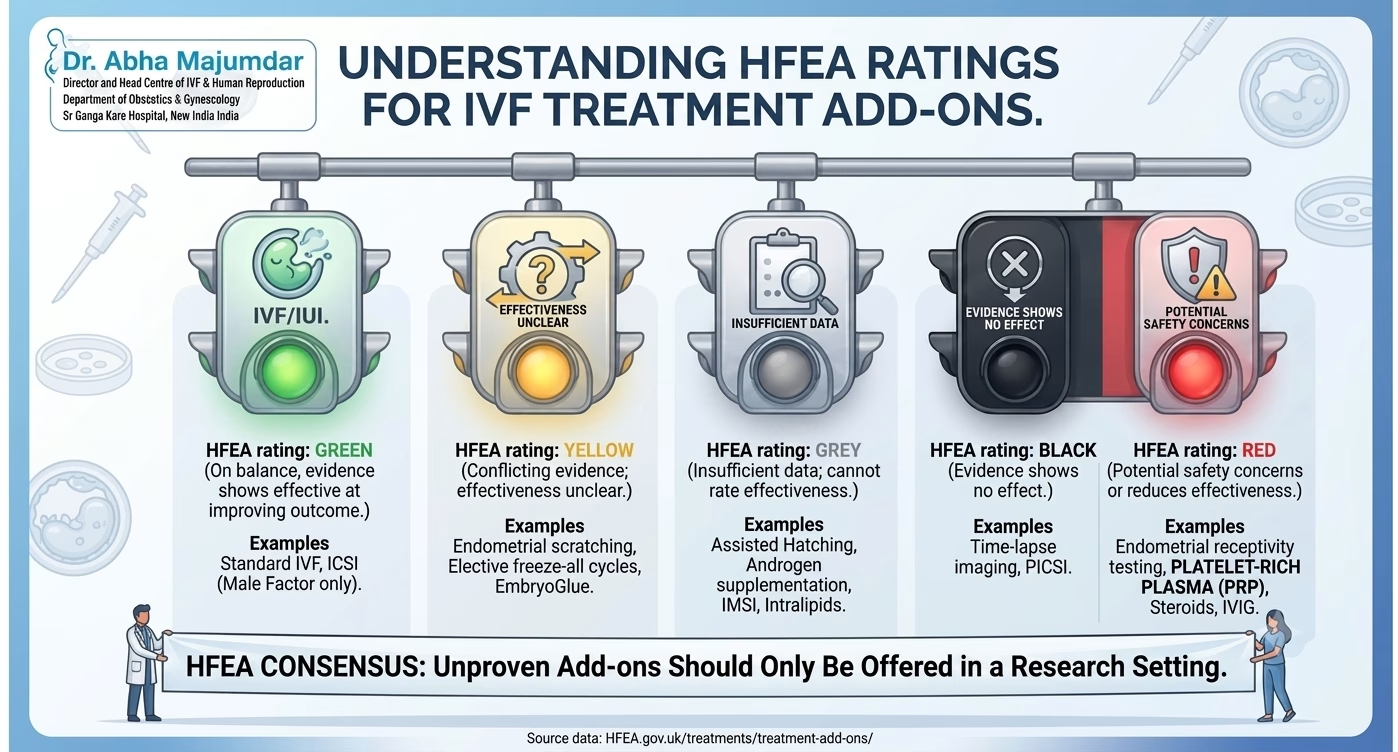
Understanding the Evidence: The HFEA Traffic-Light Ratings
To protect patients and bring transparency to the field, the HFEA’s Scientific and Clinical Advances Advisory Committee (SCAAC) reviews published data and categorizes common add-ons using a strict traffic-light rating system. When clinics routinely suggest these procedures, patients must understand where they stand on the scientific spectrum:
🟢 Green: High-quality evidence shows this add-on is effective at improving treatment outcomes. (Notably, no routine add-ons carry a green light for general use).
🟡 Yellow (Conflicting Evidence): It is not entirely clear if the add-on is effective because moderate-to-high-quality studies show conflicting results. Examples: endometrial scratching, elective freeze-all cycles, and Hyaluronate-enriched pre-transfer culture medium (e.g., Embryo Glue).
🔘 Grey (Insufficient Evidence): The effectiveness cannot be verified due to a lack of high-quality data. Examples: Assisted Hatching, Androgen supplementation, Intracytoplasmic morphologic sperm injection (IMSI), and Intralipids (immunological therapy).
⚫ Black (No Effect): Moderate-to-high-quality evidence explicitly shows this add-on has no effect on improving the treatment outcome. Examples: Time-lapse imaging a, and physiological intracytoplasmic sperm injection (PICSI).
🔴 Red (Safety Concerns / Decreased Effectiveness): High-quality evidence indicates potential safety risks or shows that the add-on may reduce the effectiveness of your treatment. Examples: Endometrial receptivity testing, steroids (Glucocorticoids), Intravenous immunoglobulin (IVIG), and Platelet-rich plasma (PRP) treatments (both intraovarian and intrauterine).
When is it Appropriate to Use a Treatment Add-on?
This evidence should make all of us pause, but it does not mean add-ons have no place in medicine. There are valid nuances to consider:
Justifiable Medical Redirection: An add-on may be offered for reasons other than simply increasing the live birth rate. For example, specific protocols might be justified if they significantly reduce the risk of a miscarriage such as with natural ovulatory cycle for frozen embryo transfer or mitigate the threat of Ovarian Hyperstimulation Syndrome (OHSS) in a specific high-risk patient by using antagonist protocol with agonist trigger and freeze all policy.
Strictly Monitored Subgroups: Certain procedures are authorized only for highly selected cohorts. For instance, ‘Artificial oocyte Activation by using Calcium Ionophore carries potential chromosomal risks and is not meant for routine use, but it may be justified for patients with specific cellular deficiencies (like PLC zeta deficiency) or those with severe, repeated fertilization failure.
Research only: Treatments that lack strong evidence of safety or effectiveness ‘should only be offered within formal research setting or clinical trial’. Crucially, patients should never be charged extra to participate in research.
Scientific Framework & References
Human Fertilisation and Embryology Authority (HFEA). Fertility treatment add-ons: a guide for patients and consensus ratings. UK Government Regulatory Review 2023.
Harper J, Jackson E, Radmann K, et al. Adjuncts in the IVF laboratory: where is the evidence for IVF add-ons? Human Reproduction 2017;32(3):485-491.